
Ruben Nava, MD is a lung transplant surgeon and researcher in the thoracic immunobiology laboratory at the Washington University School of Medicine Division of Cardiothoracic Surgery. He and colleagues published a research article in the March 21, 2024 edition of the Journal of Clinical Investigation. The study focused on a persistent question concerning the immune response to organ transplantation. In organ transplant surgery, patients require immunosuppressive medication to ensure the newly grafted organ thrives. In the article, Nava investigates the immune response that occurs in lung transplantation and the signaling proteins responsible for the development of ischemia-reperfusion injury which has been linked to organ rejection.
“Currently, primary graft dysfunction has no treatment; there are only supportive measures,” says Nava, an Associate Professor of Surgery in the Division of Cardiothoracic Surgery. “But it is very ineffective.”
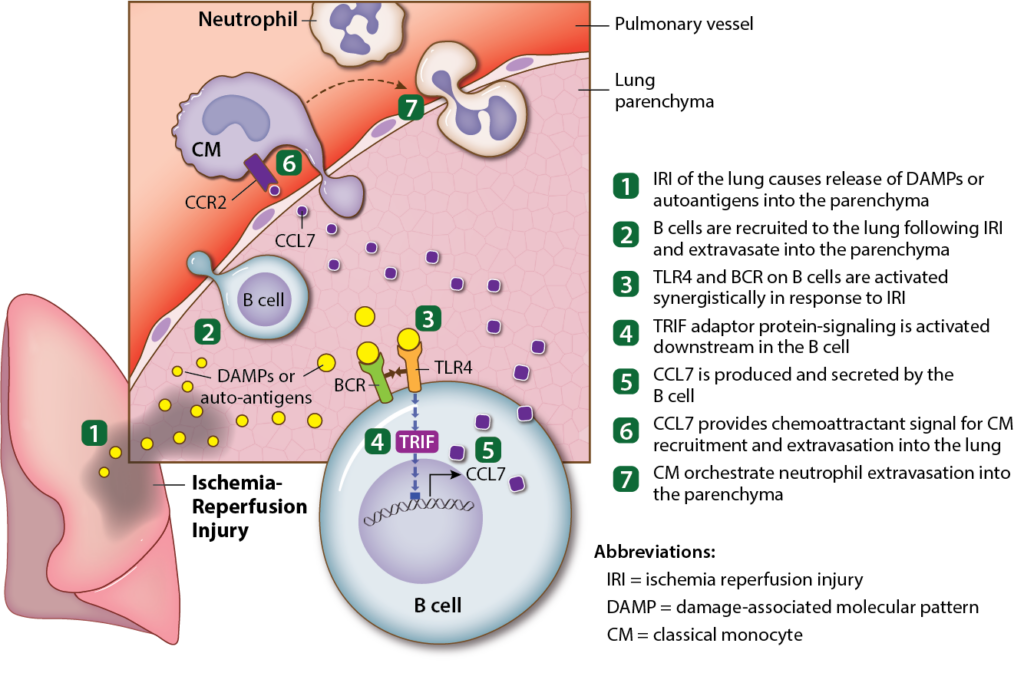
In lung transplantation, a problem arises in which the lung tissue suffers from a reaction to the lack of blood flow and subsequent reintroduction in what is known as lung ischemia-reperfusion injury (IRI). Ischemia is the period between the harvesting and restoration of blood flow to an organ. When the lung is reintroduced and revascularized, it has an immediate immune response. B cells (a type of lymphocyte, commonly known as white blood cells) are recruited in high quantities, activating an inflammatory response that worsens lung injury.
“For a long time, it was believed that neutrophils were the first innate immune cell type to arrive to the lung after ischemia-reperfusion injury. However, reports from our group showed that monocyte arrival precedes that of neutrophils. This study extends these observations by demonstrating that B cells arrive even earlier than previously thought and describes a role for B cells as critical orchestrators of lung ischemia-reperfusion injury,” says Nava.
“Lung transplant is the only treatment option for patients who have end stage respiratory failure,” says Nava. He explains that despite many advances in clinical care, along with new knowledge of the pathology and immunology of lung transplantation, t five-year graft survival remains low when compared to other solid organ transplants. “Ischemia-reperfusion injury is the main cause of primary graft dysfunction, which leads to early mortality. Its connection to chronic rejection decreases the life expectancy of this group of patients,” he emphasizes.
Translational Study
To run this investigation, Nava and his research team used murine models of ischemia-reperfusion injury including hilar clamping and lung transplantation.
“Using a variety of congenic models, we were able to differentiate the role of recipient versus donor-derived B cells and found that recipient-derived B cells are mainly responsible for the lung injury,” Nava says.
The investigators observed the models’ response, which began with the deployment of B cells, who recruited and flooded the area with classical monocytes and neutrophils within 2 hours of reperfusion. “What we found is that the immune response is largely from the transplant recipient. Up to 90% of the B cells that flood the area of injury were from the recipient, not the donor,” says Nava.
Nava and his team used staining and time-lapse imaging to record their findings. They observed B cell count in tissue, whose presence significantly increased in the lung tissue one hour after blood flow was restored.
A further goal of this study is the identification of specific signals that trigger the inflammatory immune response. “Understanding which signals are responsible for recruitment and activation of B cells immediately after reperfusion will be instrumental to developing targeted therapeutic treatments to mitigate IRI,” says Nava. “Additionally, we found that B cell depletion prior to hilar clamping in one of the murine models proved to reduce injury. Currently we do not use this type of treatment in human transplant recipients, but we hope that our findings will be implemented clinically in the future.”
Further Investigation for Long-term Outcomes
“There is potential for a human trial in which we deplete B cells in transplant recipients prior to transplantation,” says Nava. “This is already a therapy that is used in cancer patients.” Nava explains that there have been similar trials in kidney transplant patients, in which the B cell depleting agent was provided after transplantation, but not prior to transplant. “We propose that the depletion agent needs to be provided to the transplant recipient before surgery, so that none of those cells are present in the graft after reperfusion to cause injury,” he says.
Nava is preparing a grant proposal for a further investigation that will target the role of those activated B cells after IRI.
“There have been many studies into the role of B cell receptors in the setting of pathogenic infection, but not in sterile responses,” he explains. “After finding out that B cell receptors are activated without the presence of pathogens, we hope to address the question of what is the final fate of those B cells—do they become antibody producing cells, memory B cells, or are they going to be reactivated at a later point,” he explains.
Nava adds that such an investigation might determine whether those same B cells cause graft failure at a later time, if triggered by infection.