Diverticulitis is the inflammation or infection of diverticula, small pouches commonly occurring in the colon. Diverticulitis causes abdominal pain, fever, nausea and a changes in bowel habits. Mild diverticulitis can be treated with rest, changes in diet and use of antibiotics, but severe or persistent attacks of diverticulitis requires surgery. Diverticulitis is considered a lifelong condition that requires vigilance to prevent complications. Surgeons at Washington University School of Medicine in St. Louis, including Kerri Ohman, MD, treat patients with severe diverticulitis. Dr. Ohman answers questions about the progression, diagnosis, treatment and recovery from this condition.
What is diverticulitis? Is it different from diverticulosis?
Diverticulosis and diverticulitis are related but different conditions. Diverticulosis is defined as the presence of “diverticula” or small tissue pouches similar to hernias in the lining of the digestive system, most often in the lower part of the large intestine (colon). Diverticulitis occurs when one or more of the diverticula burst, leading to infection or inflammation. Diverticula and diverticulosis are common, especially after age 40, and are usually benign with no symptoms. Diverticulitis, however, arises in about a quarter of patients with diverticulosis.
What causes diverticulitis? What are the risk factors?
Diverticulosis, or the presence of diverticula, is common in those who have a low-fiber, high fat diet. In general, diverticula and diverticulosis result from high pressures in the colon, often related to the typical Western diet. These pouches are weak spots in the colon susceptible to bursting, which then causes diverticulitis. Doctors do not understand what actually causes a diverticula to burst, but it may be related to the same life habits that contribute to diverticulosis.
Risk factors for developing diverticulitis include:
- Age
- Obesity
- Smoking
- Low activity levels
- Low fiber, high animal fat diets
- Medications including steroids, opioids and nonsteroidal anti-inflammatories (i.e. Advil, Motrin)
What are the symptoms of diverticulitis? Are there complications?
Common symptoms from diverticulitis include lower or left-sided abdominal pain accompanied by fever. Lower abdominal tenderness is also a diagnostic symptom. Other symptoms include nausea, vomiting, constipation or diarrhea. Some patients experience chronic symptoms, like pain during bowel movements.
Complications from diverticulitis include abscesses in the diverticula, causing pus to collect in the pouch. Bowel blockages can also result from the scarring of burst diverticula, or these perforations can lead to fistula (abnormal passageways through the tissue). Peritonitis can progress from these ruptures or fistula if contents of the intestine enter the abdominal cavity.

How is diverticulitis diagnosed?
Diverticulitis is usually diagnosed after an acute attack, or the initial rupture of a diverticula. A doctor will conduct a physical examination, which will include checking your abdomen for tenderness and possibly a rectal exam. To definitively diagnose diverticulitis, a CT scan is necessary. In patients who have had previous CT-proven attacks of diverticulitis, this continued diagnosis is often made based on health history and symptoms. Blood and urine tests will be conducted to check for signs of infection related to diverticulitis.
Abdominal pain can indicate a number of problems, so the doctor will need to rule out other causes for these symptoms. Other tests include:
- Pregnancy tests to rule out pregnancy
- Pelvic examination to rule out pelvic disease
- A liver enzyme test to rule out liver-related diseases
- A stool test to rule out infection in people who have diarrhea or abdominal pain
- Colonoscopy to rule out sores, ulcers or other problems related to changing bowel movements
How is diverticulitis treated?
Mild diverticulitis attacks or episodes are usually treated with oral antibiotics and bowel rest. Antibiotics are not always required in very mild cases, and patients will often improve with dietary modifications. Bowel rest can mean drinking only clear liquids or eating a “low residue” diet, reducing both fiber and fat.
For more severe diverticulitis, patients may be hospitalized and need intravenous antibiotics. More severe complications require complete bowel rest, meaning the patient cannot eat and instead receive intravenous fluids and nutrition.
Sometimes, patients develop abscesses or pus collections around their colon that require percutaneous drainage. A radiologist will administer a drain through the skin into the abscess cavity to drain the abscess.
The most severe manifestation of diverticulitis results when there is a free perforation of the colon into the abdominal cavity, causing peritonitis. This is a life-threatening situation requiring emergency surgery and frequently the creation of a temporary colostomy. For patients who have recurrent attacks of diverticulitis, elective surgery may be recommended.
What forms of diverticulitis treatment require surgery?
Surgery to treat diverticulitis becomes necessary for:
- Multiple episodes of uncomplicated diverticulitis
- A complication related to diverticulitis, such as a bowel abscess, stricture, fistula or obstruction
- A weakened immune system
- A puncture (perforation) in the bowel wall, leading to peritonitis and emergency surgery
There are two main types of surgery. Primary bowel resection is when a surgeon removes the affected part of the intestine and reconnects the healthy segments, allowing the patient to have normal bowel movements. This may be an open surgery or a minimally invasive (laparoscopic) procedure, depending on how large the affected area is.
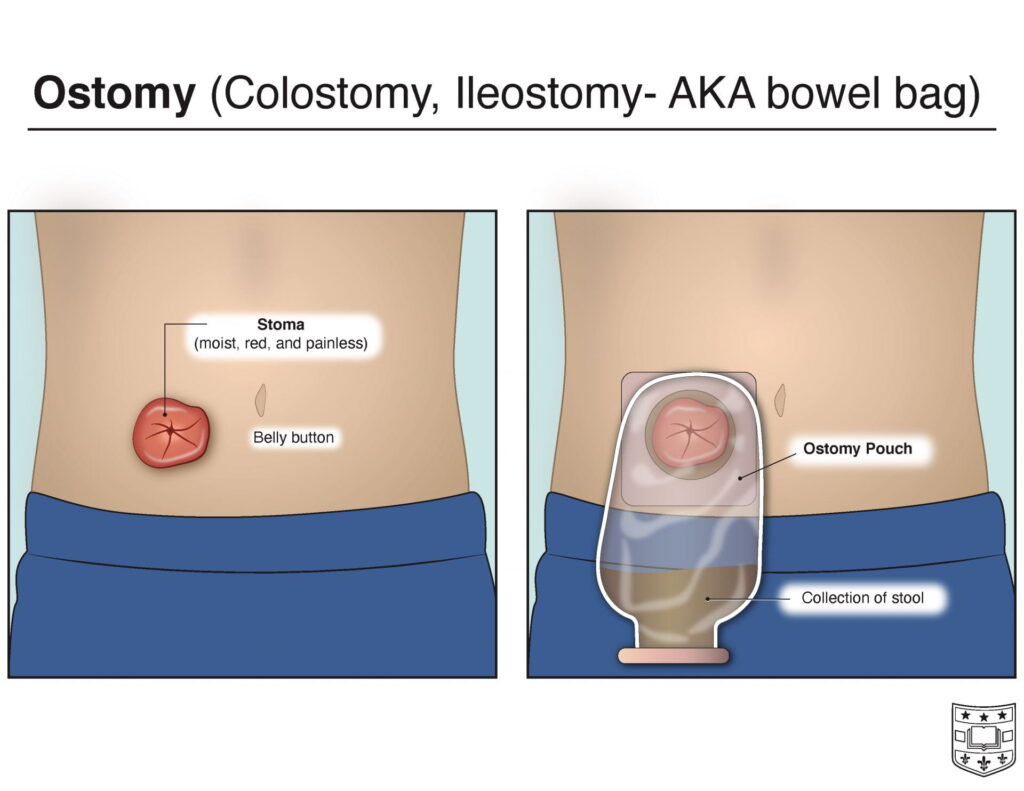
Bowel resection with colostomy may be performed when inflammation makes it impossible to rejoin the colon and rectum. An opening (stoma) in your abdominal wall is connected to the healthy part of your colon. Waste passes through the opening into a bag. Usually, when a colostomy is necessary in these situations, it is temporary. Colostomies may be necessary when patients have had extremely severe attacks or have developed extremely complex fistulas. If emergency surgery is required in cases of complete perforation and peritonitis, a colostomy is frequently necessary. This is usually a temporary colostomy and it can be reversed several months after the patient has recovered. Once the inflammation has eased, the colostomy may be reversed and the bowel reconnected.
For patients with recurrent disease, surgery is frequently recommended after three or four attacks. The recommendation for surgery depends on many factors, including the severity of the attacks, the frequency of the attacks, and the patient’s willingness to suffer from these repeated attacks.
What is recommended for recovery from or prevention of more severe diverticulitis?
After recovery from diverticulitis, a high-fiber, low-fat diet is the best diet. There is also evidence that this can reduce the risk of subsequent attacks. High-fiber diets, including fresh fruits and vegetables and whole grains, decrease diverticulitis risk. Exercising regularly, around 30 minutes five times a week, promotes healthy bowel function and reduces the pressure that occurs in the colon. Drinking adequate amounts of fluids replaces the water absorbed by a high-fiber diet, as too much fiber can be constipating if it isn’t matched with the correct amount of fluids.
If a patient has an attack and has not had a recent colonoscopy, a follow-up colonoscopy should be performed a couple of months after recovery from the diverticulitis.
What should a patient do for a diverticulitis attack?

For mild attacks, the patient should call their physician, but more severe attacks may require emergency room attention. Quick action is necessary when symptoms are more severe or persistent, as these may indicate a complication or infection that needs immediate treatment.
Washington University Diverticulitis Treatment
Physicians at Washington University Section of Colon and Rectal Surgery can provide treatment options for diverticulosis or diverticulitis. Dr. Ohman and the Colorectal team are dedicated to patients requiring care for this and many other conditions. Contact our specialists here.