Car wrecks, falls, acts of violence and sport-related accidents are some of the most common causes of cervical spinal cord injury (SCI). The cervical spinal cord is the top part of the spine, located in the neck, and consists of the C1-C7 vertebrae. SCI is a devastating, life altering injury that damages the nerves connecting the brain to the rest of the body. Depending on the location of the injury, SCI can leave a person partially or completely paralyzed.
In July of 2019, Ida Fox, MD, Associate Professor of Plastic and Reconstructive Surgery, was invited to review and write the commentary for a case series published in The Lancet. The case series, authored by Natasha van Zyl, observes the outcomes of two types of procedures used to restore upper limb movement to people with SCI: tendon and nerve transfer.
Fox, a peripheral nerve and hand and wrist surgeon at Washington University School of Medicine and Barnes-Jewish Hospital, knows these procedures well.
Tendon transfer surgery helps to restore function by using a muscle in the arm that is still functioning, and connecting that muscle to others that are not. Because there are multiple muscles that are able to perform the same function, such as bending the elbow, surgeons can take a redundant muscle for this purpose. Tendon transfer is like “tying ropes together,” Fox describes, so that the individual can mechanically manipulate their hand by moving the functioning arm muscle.
“Tendon transfer creates something like an internal pincher or power gripper,” Fox says.
Nerve transfer surgery is a newer tool for people with SCI. Similar to tendon transfer, nerve transfers use something that is working, but extra. If there are nerves in the arm that connect to the brain above the level of SCI, the brain can still talk to those nerves. Fox transfers a functional nerve to the hand, making it possible for the hand and brain to communicate again. If tendon transfer is like tying together ropes, nerve transfer is more similar to rewiring a circuit.
“Nerve transfer,” Fox observes, “tends to offer more fine motor skills, control and dexterity.”
As opposed to a power gripper with an opening and closing function, nerve transfer allows the individual more natural finger movement.
“In both tendon and nerve transfer, we restore function using the tools and parts available,” Fox says. “Restoring form and function is what plastic and reconstructive surgeons do.”
Actions most people never think twice about—shaking hands or lifting a water bottle—become awkward and difficult, if not impossible, for people with cervical SCI that limits their upper extremity function. Tendon and nerve transfer offer subtle but important changes in motion, giving individuals new independence. The literature says that many people rank hand movement as more important than sexual function or the ability to walk.
“For people without hand function,” Fox says, “a little goes a long way in terms of their independence.”
According to Fox, though, which procedure is best depends on the person.
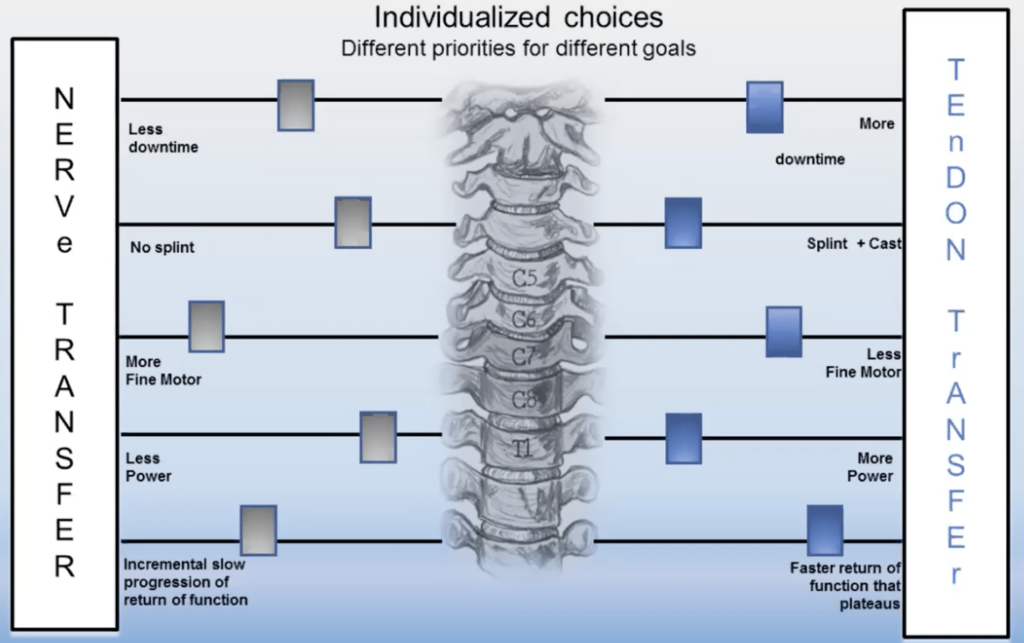
In her Lancet commentary, Fox writes that, in her experience, “each person with spinal cord injury responds uniquely, and injury patterns, clinical examinations, electrodiagnostic testing, social situations, and functional goals are diverse. Shared physician-patient decision making is imperative to develop a plan that meets an individual’s expectations and biopsychosocial situation.”
Nothing Is Ever Black and White
Fox, who is Co-Director of the Center for Nerve Injury and Paralysis, completed her medical training at University of Rochester Strong Memorial Hospital, where she first worked with people who had SCI, performing flap procedures to treat pressure sores, many of whom had injuries of the spinal cord.
Fox learned another important concept while at Rochester: biopsychosocial medicine.
“Practicing biopsychosocial medicine means doing what’s right for the right person at the right time,” Fox says. This means seeing more than the physical aspects of an individual’s condition. Fox accounts for the person’s psychological status—their goals, expectations and feelings—and social circumstances. Important social aspects for someone with cervical SCI might include their level of caregiver support, access to resources during the recovery process, insurance coverage and the ways in which they will use their hands after the surgery.
Biologically, some people might not be candidates for one or either surgical option. Psychologically, the individual’s goals and the reality of what surgery can offer must align. Socially, there has to be the proper support system in place to achieve recovery and positive results. Applying a biopsychosocial approach to patient care has helped Fox provide the best care for each person, whether they receive nerve or tendon transfer, or no surgery at all.
“Ida Fox is providing such a necessary service for individuals with cervical spinal cord injury,” says Division Chief Justin Sacks, MD, MBA. “This work builds on the division’s strong history of groundbreaking research and clinical care in nerve reconstruction.”
Sacks recognizes the incredible value of nerve transfer surgery for people with cervical SCI, and the important innovations in the area driven by his predecessor, Susan Mackinnon.
“Susan Mackinnon revolutionized the field of peripheral nerve transfer,” Fox says of her early mentor at the School of Medicine.

Susan Mackinnon, MD, former Chief of the Division of Plastic and Reconstructive Surgery, and recipient of a 2020 Distinguished Educator Award from the School of Medicine, is a pioneer of nerve surgery. Fox recalls Mackinnon performing the first nerve transfer surgery for a person with SCI. Tom Wachtel, a trauma surgeon injured in a devastating car accident, was left quadriplegic. At the time, it was uncertain how much nerve transfer could help a quadriplegic person. Nine months passed before Wachtel wiggled his finger and thumb—feats previously impossible for him. From there, he continued to regain function as he recovered, garnering Mackinnon and the School of Medicine international attention.
After this groundbreaking procedure, Mackinnon knew the division would see more cases—they had discovered a way of restoring function for individuals who previously had no options. The medical school needed someone to take on nerve transfer for SCI, which would become a vital service for people in need.
Fox stepped up.
She had experience with SCI, she had studied nerve transfer with Mackinnon and she had the sensitivity to understand biopsychosocial needs of her patients. Fox met with other experts, collaborated with her colleagues in plastic and reconstructive surgery and identified the need for a multidisciplinary team, including therapists, SCI physicians, people with cervical SCI and caregivers, fellows, nurses, neurologists and researchers.
Today, her research focuses on helping people make informed choices about their treatment. Fox is the principal investigator on a multi-disciplinary, multi-institutional research project studying natural recovery after cervical SCI and surgical treatments to restore upper extremity function, with the ultimate goal of developing a decision aid that guides individuals through the facts of SCI and helps them make informed, evidence-based decisions that fit their goals.
Around the World
Fox’s passion for biopsychosocial medicine originates in her training at University of Rochester, but her interest in people stretches back much further. Her mother came to the United States from Japan on a Fulbright scholarship to study English, planning to return to Japan as an English teacher. Instead, she met Fox’s father, a science writer, and stayed in the United States. Fox recalls visiting Japan on rare occasions, mostly for funerals.
“We didn’t speak Japanese at home, because my mother was supposed to be an English teacher,” Fox says. “I wanted to take Japanese in college, but I was already too busy with pre-med classes and a full schedule.” The Japanese culture of her mother’s past was intriguing and curious to Fox. “I really wanted to connect with that part of my heritage.”
Her solution was to defer medical school for a year after graduating college, putting her busy life on pause. Between college and medical school, Fox lived in Japan for a year, immersing herself in the culture and experiencing something far different from what awaited her in Rochester. Fox finally learned Japanese. She stayed with family friends, taught English like her mother had trained to do, and traveled.

For part of that year, Fox waitressed at a busy restaurant with an international clientele.
“I’m good at memorizing peoples’ drinks. If I weren’t a surgeon, I would probably be a bartender,” Fox says. “I had an uncanny ability to memorize what people ordered, whether it was in English, French, Japanese or whatever language. That short-term memory was very useful in medical school!”
While working at the restaurant, Fox rented a small apartment in Tokyo. “Basically, it was an expensive closet with a curtain instead of a door,” she says. The apartment was far from ideal, but it allowed her to stay close to the culture, experiencing life in Tokyo and work in a thriving, worldly environment. “I was having so much fun, meeting so many people from all over the world and speaking all of these languages.”
Balancing Act
When she returned home, Fox brought with her a world of experience. She had reconnected with a distant part of her family, and would soon start a family of her own. She studied medicine at Rochester, and with Mackinnon at Washington University, then joined the faculty in the Division of Plastic and Reconstructive Surgery. In Fox’s mind, the decision to stay at Washington University was an easy one.
“There are very few places in the country where you can practice at a center that does level 1 trauma, oncologic, transplant, reconstructive and nerve transfer surgery. In most big cities, these services are all divided up,” Fox says. “Washington University and Barnes-Jewish Hospital are a perfect fit for me, because I want to do it all.”

Family is another deciding factor for Fox, who has a husband and daughter. Life for Fox is busy, and she acknowledges that things are not always in perfect balance—she and her husband prep a week worth of meals at a time and have to eat the same thing for breakfast and dinner each day; her home office is a bit of a mess—but she is providing care that greatly improves the lives of individuals with SCI, and she has the time to spend with her husband and daughter.
“My daughter is going to be young once,” Fox says. “I try to focus on what’s important. At Washington University, there’s a very human mindfulness for what matters. It’s hard at times, being a busy surgeon, but in the long run you find balance.”

Fox brings that delicate balance to work, where she helps patients make informed choices about their care. She is excited by the possibilities of nerve and tendon transfer surgery for patients with SCI, but also emphasizes the importance of finding the right solution for each person. “We hope,” she writes in concluding her commentary for The Lancet, “that increased awareness of nerve transfer surgery will stimulate early referral, wide discussion, and appropriate use of this treatment option throughout the world.”